
According to the statistics, there are around 13,000 practising SLPs in the UK and around 2.5 million people in the UK have a speech or language difficulty:
- 5% of children enter school with difficulties in speech and language
- 30% of people who have had a stroke have a persisting speech and language disorder.
In terms of the functional duties of a speech therapist, we can single out one very significant duty that should not be overlooked. This is the completion of the necessary documentation in the prescribed form to meet the demands of a huge number of these people. A clinician's ability to manage it is one of the most important indicators of their professionalism.
A therapist devotes a lot of time to writing session notes, conclusions, characteristics, representations, and the design of speech cards. Thus, he should use his working time rationally.
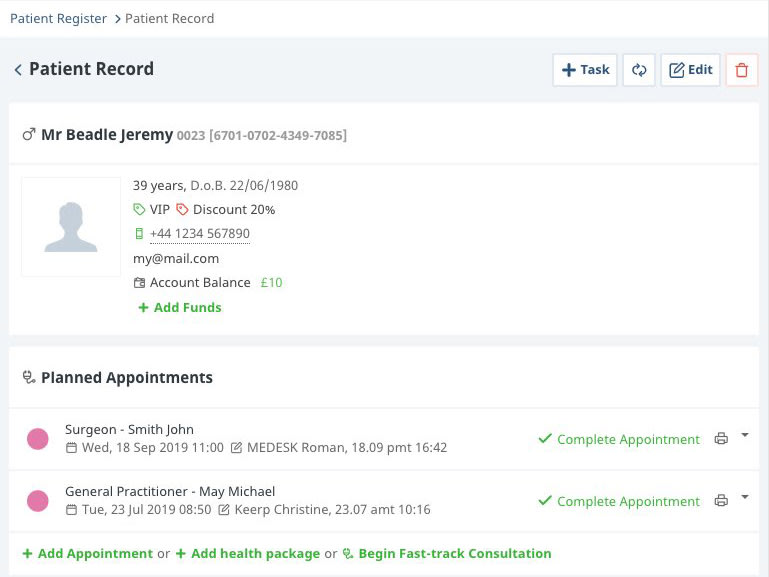
Learn how to simplify your practice workflow and free up more time for patients with Medesk.
Open the detailed description >>When identifying children with peculiarities not only regarding speech development, he makes suggestions for further successful plan of care, or, if necessary, refers them to a specialist (neuropsychiatrist, neuropathologist, otolaryngologist, etc.).
Therefore, in order to save more time on the selection of the necessary phrases, special expressions, and formulations, we have selected a few suggestions for daily notes that simplify filling out the documents, while maintaining their content and accuracy. As a result, they are better able to organize their work and develop their skills in the field of speech-language pathology.
A SOAP note format is one of the most effective ways to fill out a progress note. We are planning to teach you how to use this tool in your private practice. In addition, we are going to give you some lifehacks and tips that will make the client's progress a reality.
SOAP Note Format for Speech Therapy Sessions: What is It?
SOAP notes are widely used by various specialists: mental health professionals, psychologists, caregivers, and speech-language pathologists.
When filling out a document for clients, it is necessary to know the content of regulatory documents related to this issue. It is also necessary to remember the age and individual characteristics of the person based on his diagnostic data, and take into account the results of speech development.
This information is included in the soap note template.
#1. S is for Subjective
The subjective section contains information about the actual state of the patient. Ideally, this part of the notes should be as true to life as possible. What does it mean?
The doctor keeps track of the complaints and speech issues of the patient, as well as other significant information about the patient. He must report only the words of the clients, but not his own thoughts and ideas. It’s not the time for it.
The first priority is to take stock of symptoms and make up a potential and theoretical treatment plan (but not to put it down). Try to use direct speech.
More frequently, the clients of speech pathologists are children, accompanied by their parents. So, sometimes you listen to both of them.
Medesk helps automate scheduling and record-keeping, allowing you to recreate an individual approach to each patient, providing them with maximum attention.
Learn more >>For example, you can mention:
- Mrs. Smith (Billy’s mother) claims that the child has speech development problems.
- "The child suffered pneumonia at an early age."
- The mother claims that the child prefers to work with his left hand.
- "I find it difficult to come up with a word for a given sound."
- "Billy has been stuttering since he was 3 years old."
- "He is inconsiderate and impulsive."
#2. O is for Objective
The objective section of the notes contains your thoughts, prognoses and conclusions as a professional. The name of the section makes it pretty obvious. Test results, questionnaires, physical examination, fine and gross motor skills, articulation and tempo, speech intelligibility, breathing characteristics, and any other measurable indicators should be included in this section.
You can also provide some additional information (brief – psychological and pedagogical characteristics), if applicable.
The main rule is to avoid value judgments and be completely unbiased.
In the table below you’ll find different aspects to include in the objective part of a treatment note and some examples of possible answers.
Examples of comments (the Objective section)
| Mobility of the articulatory apparatus | The state of fine and gross motor skills | Sound reproduction | Vocabulary | Writing | Reading |
|---|---|---|---|---|---|
| Can hold the articulatory position for a sufficient time | The motor skills of the hands’ small muscles are not sufficiently developed; | Pronunciation shortcomings; | The amount of vocabulary corresponds to age; | There are numerous errors of various kinds; | The method of reading letter – syllabic; |
| the movement of the tongue is slow, with difficulties | arbitrary motor skills are not formed; | the pronunciation of sounds is broken ...; | the dictionary is poor, inaccurate, limited to everyday topics; | has difficulties in mastering writing and reading | slow reading, syllabic, in words; |
| during articulation exercises, muscle tension increases; | the leading hand is the right; | defectively pronounces oppositional sounds; | has difficulties in selecting antonyms, synonyms, single-root words; | when writing off, single errors are observed; | reading comprehension with inaccuracies; |
| the tip of the tongue is inactive. | performs all movements correctly; | disadvantages of pronunciation of voiced consonants (deafening); | often uses nouns, verbs, pronouns, less often – adjectives, adverbs. | when writing under dictation, he makes many mistakes (omissions, additions, omissions of prepositions, merged spelling of words). | reading is syllabic, reads simple words holistically; |
| difficulties are noted when performing exercises for the dynamic organization of movements. | pronounces all sounds correctly in isolation, but with an increase in the speech load, there is a general blurring of speech. | makes hesitations when reading polysyllabic words. |
#3. A is for Assessment
The assessment section summarizes the achievements of two previous sections. Note-taking at this stage includes analysis of subjective and objective information and interpretation of the whole session.
Now you are finally free to use professional terms and acronyms, as this part of the notes is for professional use only. And if you aren’t able to continue the therapy, a substitute therapist will easily know what to do thanks to your notes from the last session.
Discover more about the essential features of Medesk and claim your free access today!
Explore now >>It should be noted that there is no need to repeat the S and O sections. And also, it’s a bit early to make plans - just wait for the next stage and follow the SOAP structure.
As an example, we give you some assessments of the difficulties of educational material’s assimilation (a child in a primary school):
- Difficulties of adaptation in a school institution;
- Violation of motor skills in the form of insufficient coordination of movements;
- Pedagogical neglect due to unfavorable social conditions of the child;
- Disadvantages of attention, emotional-volitional regulation, self-control;
- Motor disinhibition, hyperactivity;
- ADHD;
- Verbal and logical thinking is poorly developed;
- Insufficient development of coherent speech;
- Neurotic and neurosis-like states (fears, tics, mild stuttering, enuresis, etc.)
#4. P is for Planning
The last stage of note-taking is creating future plans for treatment. The plan section contains goals and recommendations for the follow-ups, even some handouts, since the plan is for a client and other healthcare professionals, who will take part in his treatment.
When writing any kind of counseling notes, set goals in the final section and make sure they are realistic and measurable. It's vital for a patient to remain motivated and to believe in recovery. You can easily split the goals into small ones to make a client’s performance and progress more transparent.
Moreover, the plan makes arranging individual sessions easier. Therefore, as a professional who wishes to get the greatest profit for given help, you increase your chances of setting up the next session.
As a bonus, we’ve collected some recommendations you can include in the plan stage:
- Avoid intellectual and psychological stress;
- The child needs an individual approach and constant supervision by adults;
- In order to compensate and equalize the shortcomings of physical, mental and speech development, avoiding overloads, it is recommended to repeat the course of study (or study in a special correctional school);
- It is recommended to consult with specialists...
- Additional rest is recommended;
- Conducting an additional examination in order to determine the child's need for further education, taking into account his level of development;
- The child needs step-by-step guidance and frequent changes in activities;
- Continuation of speech therapy classes according to the schedule 2-3 times a week for 45 minutes;
- Attending a special (correctional) school;
- Classes with parents aimed at developing motor functions, designing, classifying, viewing pictures, reading fairy tales, playing the story; plot-role-playing games; fixing the use of gestures for communication; development of auditory perception (differentiation of sounding toys, sounding pictures in books), onomatopoeia.
Electronic SOAP Note Example
The SOAP format of making notes has proven itself as a convenient, simple, but effective technique.
But do you remember that you should make notes during every session?
Though filling four sections of a note is rather simple, it takes a lot of time and strength to do it manually.
For professionals with a large patient flow (and we are sure, you belong to this category), the use of Electronic Health Records is a must.
The benefits of the software are obvious:
- All necessary stages of your future notes are pre-set for you (with templates ready to be printed)
- You can use an autofill option for the most general data
- The interface is easy and makes it possible to fill out the information right during the session with minimal distractions for the patient.
- It's unreal that the notes have been lost. All data is securely stored.
A good SOAP note is the result of the thorough work of a speech specialist. But you can make your practice much easier by implementing EHR in your therapy service.
")

![How to Start a Physical Therapy Clinic in 2025 [10 Easy Steps]](/i/6mBjkkKkX3WbXuafkOkdbf/78dc8966e27eb239329dc39d569ab8bb/how-to-start-a-physical-therapy-clinic-svg.svg?w=747&h=473&fit=fill&bg=%23DEDEDE "How to Start a Physical Therapy Clinic in 2025 [10 Easy Steps]")